
Proceedings of the International Symposium On penile Disorders.Hamburg, Germany, January 26-27, 1996
Enhancement Phalloplasty with Girth Augmentation by Autologous Fat Transfer : A Further Report of 700 Cases
It is possible by surgical means to enhance the length and girth of the pendulous penis. Previously, we reported our experience with our first 162 patients. The purpose of this paper is to document our experience since June 2, 1992, with around 700 enhancement phalloplasty procedures.
Masters and Johnson note that « the size of the male organ both in flaccid and erect state has been presumed by many cultures to reflect directly the sexual prowess of the individual male ». Widely diverse cultures, ancient and modern, have linked penis size to virility, dominance, and power. Even among the affluent and well-educated, penis size often equates to manliness. Few men, including those presumably indifferent to penis size, would wish to have a smaller penis. If a man’s perception is that his penis is too small, it will matter littIe to him when his surgeon assures him that he is normal or average. Feelings of inadequacy and low self-esteem often influence, even dominate, his personal and occupational relationships.
The nature of the operation and its exploitation by surgeons promising unrealistic results have unclerstandably provoked the opposition of surgeons whose training is traditionally directed toward improving physicai function or correcting pathology. The argument is advanced that if a man’s penis is already normal there can be no justification for his wanting to be larger. Feelings of inadequacy and poor self-esteem are not manly and are matters more appropriate to the psychiatrist’s couch than to the operating room. Yet plastic surgeons routinely deal with issues of image and self-esteem 1. There may also be the unspoken suspicion that a man overly concerned with the size of his penis is probably homosexual. In fact, the vast majority of our phalloplasty patients are heterosexual. Most candidates are aware that they have penises of normal or average dimensions. Interestingly, most patients have never suffered disparaging remarks from their sexual partners.
Their desire is to improve their locker-room appearance. Many of our patients are body builders and weight lifters who are committed to obtaining a highly developed, idealized vision of themselves. Such men often are not satisfied with an average or normal penis. Other patients have suffered youthful ridicule and humiliation from other males over undersized penises. Our first patient had attempted suicide twice before he and his parents consulted us in June 1992. Such patients may become reclusive and avoid relationships and situations where their bodies become exposed. These patients are often the most grateful for even modest gains… Many men come seeking the operation who are obsessed with the most minute details of their physical appearance.
Questioning will often reveal deep-seated feelings or inadequacy. Our experience is that no matter the results, these patients will be dissatisfied. No matter how perfect you make their penis, it will never be pertect enough. Such patients should not undergo surgery. Dissatisfied patients can be vociferous, vituperative, violent, and vindictive.
Various studies have indicated that the average erect penis is between 13.8 – 16.6 cm. Caucasians and Blacks are comparable in the erect state. In the flaccid state Blacks appear to average about a centimeter longer. Asians are smaller, a fact taken into account by manufacturers of penile prostheses and condoms. Patients with abnormally small penises, including true micropenis, can be helped significantly. Micropenis is delined as a penis size less than 2 standard deviations from the mean. For adults, this is stretched or erect penis length of 9.3 cm. The so-called concealed, buried, or retracted penis is a consequence of too much skin having been removed during circumcision and / or the presence of an overhanging hypertrophic suprapubic fat pad (see Fig. 1).
 Fig 1 • True congenital micropenis
Fig 1 • True congenital micropenis
History
The earliest references to penile lengthening techniques are found in the pediatric urology literature. These variously describe resection of the suspensory ligament, release of restricting bands of Scarpa’s fascia, suprapubic lipectomy and tethering the dermis at the base of the penis to the pubic periosteum or proximal tunica albuginea. Our own independent recognition of the possibilities for penile lengthening stems from the mid-1980s when, upon dividing the suspensory ligament during insertion of penile prostheses, we noted an apparent increase in the length of the pendulous penis. Likewise, following ligament transection during proximal ligation of their deep dorsal vein for venous leak, several patients volunteered the information that their penises appeared Tonger. Subrini reported a mean gain of 3 cm in 49 patients after release of the suspensory ligament. Furlow also described length increases in prosthesis patients after dividing the suspensory ligament.
Incisions
Acivancement of the penis requires some sort of lengthening incision. At the base of the penis all incisions except the transverse cut across skin creases and, while necessary for function, are more or less undesirable for appearance. We have at various times tried M-incisions, single Z-plasties, multiple Z-plasties, and inverted V-Y advancement techniques. We have found the V-Y advancement technique to be preferable. It is simplest and provides adequate length.
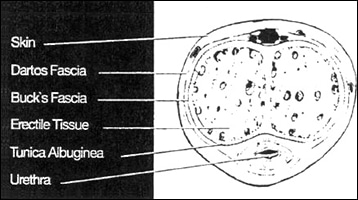 Fig 2 •
Fig 2 •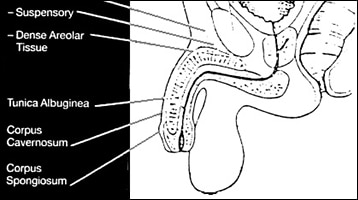 Fig 3 • Ligamentous Attachments (Fig. 2, 3 )
Fig 3 • Ligamentous Attachments (Fig. 2, 3 ) The pendulous penis is attached to the pubic bone by dense areolar tissue and the fundiform (superficial) and suspensory (deep) ligaments. The fundiform is the extension downward of Scarpa’s and Camper’s fasciae from the rectus fascia just above the pubic symphysis to the dorsal and lateral penis. The suspensory ligament is a three-dimensional triangular sheet of dense fibrous tissue stretching from the linea alba and upper portion of the symphysis pubis and arcuate pubic ligament to the center of the penis where it fans out laterally from the dorsum. Added support of the penis is provided by the dense attachments ot the crura bilateraily to the ischiopubic rami.
The Suprapubic Fat Pad
Illouz suggested that certain zones of the body are target sites for the abnormal accumulation of « privileged » fat. In males these sites include the suprapubic region, which remains resistant to the severest dietary restriction or intensive exercise. If this area should regress during famine, when caloric intake resumes this area rapidly and preferentially reaccumulates fat. In obese men, a normal penis will often be buried beneath the overhanging suprapubic panniculus. Suprapubic lipectomy is necessary to achieve optimal penile lengthening. In our experience direct scissors lipectomy is preferred to suction lipectomy. Fat thus removed from this suprapubic area is unlikely to reaccumulate.
Girth Enhancement
According to Reed, penile girth enhancement using modern techniques was first performed by Samitier in 1989. The two techniques available for girth enhancement are dermal fat grafts (DFG) and autologous fat transfer (AFT). Our experience has been chiefly with AFT.
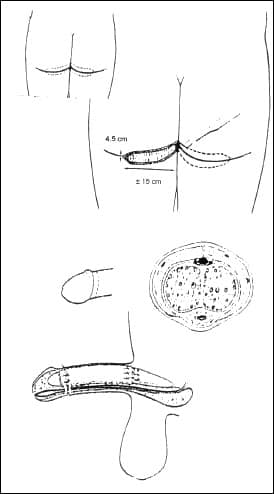 Fig 4 & 5 •
Fig 4 & 5 •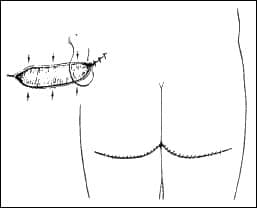 Fig 6 • Dermal Fat Grafts (Fig. 4-6)
Fig 6 • Dermal Fat Grafts (Fig. 4-6)Dermal fat grafts are composite grafts, consisting of de-epithelialized dermis and fat. Donor sites generally are from the inguinal creases anteriorly or from the medial buttock-thigh creases posteriorly. Depending on the size of the penis each donor graft is around 14 cm long and 6-12 cm wide, depending on whether one or two grafts are taken. After the grafts are removed, the incisions are undermined and closed with buried sutures, taking care to avoid dog ears. To maximize concealment the incision closure should be kept within the crease. The epidermis of the graft is stripped off the dermis and the graft thinned to about 1.5 cm. The penis is degIoved and the grafts fixed fat side down onto the dartos fascia. Some surgeons use two or more grafts placed side by side; others prefer a single large graft wrapped circumferentially around the shaft, usually stopping short of the urethra. With dermal-fat grafts almost no girth shrinkage occurs although there may be some shrink age of length. The graft may dislodge and become bunched up underneath the proximal or distal ends. If grafts are laid side bv side, longitudinal grooves may develop. The large scars created at the donor sites may be troubling, especially to devotees of the beach or the gym.
Patients may complain of incisional discomfort when they sit down. The operation itself takes most surgeons about three hours.
Autologous Fat Transfer
The usefulness of injected autologous fat for cosmetic purposes has long been vigorously debated by plastic surgeons, without consensus. In 1990 Carraway proposed the use of aspirated fat for facial contouring. Ellenbogen, in an invited comment, likened fat transfer to the emperor’s new clothes in Grimm’s fairy tale. What is abundantly clear, however, is that much of the injected fat is rather promptly reabsorbed. Peer reported that reabsorption of 50% or more of autologous transferred fat could confidently be anticipated. Chajchir and Benzaquen reported satisfactory results in most of their patients but noted that they routinely transplant 50% more fat in anticipation of partial resorption. A committee of the American Society of Plastic and Reconstructive Surgery in 1987 concluded that after one year 30% of injected fat could be expected to survive. « Therefore, overcorrection is necessary when performing fat transplants ». Fredericks raised the possibility that the survival of transplanted fat may depend on the recipient site.
Although it is unclear why autologous transferred fat survives better in some cases than in others, certain fundamental principles promoting graft survival are well known. When donor tissue, whether fat, a heart or a kidney, is removed from its native site, it becomes deprived of its nutrient blood supply. Its need for oxygen and nutrient substrate remains, but most tissues can survive by anaerobic metabolism for a limited time. Fat should transfer well since even under ideal conditions it has a relatively poor blood supply, and presumably can tolerate a higher degree of oxygen deprivation. After donor tissue is transplanted to a recipient site, there is an outpouring of nutrient-rich plasma at that site. Out of this fluid the transplanted tissue absorbs dissolved oxygen and nutrients. Within a few davs, endothelial proliferation begins, and there is a purposeful, directional ingrowth of blood vessels from the recipient sites into the donor tissues. Thick grafts take poorly because tissue death occurs before the ingrowing blood vesseis can reach the interior. Thin grafts take well because the bulk of the graft can be revascularized in a timely fashion. In the same way, large quantities of injected fat survive poorIy ; smaller amounts survive relativeIv well.
AFT takes about one hour, two hours less than DFG. There are no unsightly or uncomfortable scars. There are no longitudinal ridges. There is no loss of penile length. On the other hand reabsorption of tat is variable and sometimes uneven. There may be contour irregularities and residual nodules which sometimes do not respond to pressure. We have done a second procedure in about 12% of our patients. With AFT, unlike DFGs, if additional girth is desired later, it can readilv be done.
Factors which may contribute to survival of autologous fat are :
- Selecting patients with bountiful donor fat. Thin or muscular patients with little body fat require vigorous aspiration which may damage the fat cells and impair their take. Harvested fat is often dry, stringy, and admixed with fibrous connective tissue.
- InfiItrating the donor site with buffered (pH 7.4) physiologic solution before harvesting fat.
- Aspirating gently.
- Cleaning donor fat of detritus.
- Chilling fat until implantation.
- Dissecting gently and bluntly in recipient subcutaneous dartos tissue of penis, avoiding damage to blood vessels and Iymphatics.
- Injecting smaller (30-60 cc) rather than larger amounts of fat, depending on penis size.
- Avoid bleeding or intection at recipient site.
- Immobilizing the penis for 10 days postoperatively.
- Avoiding trauma to the penis for 6 weeks, including intercourse and masturbation.
- Refraining from cigarette smoking.
Circumcision
All uncircumcised patients are urged to undergo circumcision at least 6 weeks before phalloplasty. Simultaneous circumcision has been associated with an undesirable incidence of wound dehiscence, delayed healing, edema, and increased postoperative discomfort.
The Weight Device
After the ligaments are divided and the penis slides forward, healing begins with the formation of scar tissue. As the scar tissue matures, it contracts and tends to draw the penis back towards its original position. Before the weight device (American Bodycrafters, Huntington Beach, CA) became available every patient lost some part of the inch and a half he gained by this operation. Filling this space with liposuctioned fat does not prevent retraction and reattaching the penis seems to defeat the purpose of the operation. Using Goretex or other foreign material is unappealing because of the increased risk of infection. Injecting the area repeatedly with triamcinolone has proven ineffective. \Vith proper use of the weight device, Toss of new length is no longer a problem.
Material and Methods
Proper patient selection is the first essential of enhancement phalloplasty. The surgeon himself must evaluate the emotional stability, expectations and motivation of the patient. If there is any question, psychological consultation can be helpful. Candidates exhibiting serious doubts or reluctance, or who cling to unrealistic expectations, or who view penis enlargement as the panacea for all their problems, should not undergo surgery. No one should be persuaded or talked into surgery. The vast majority of stable, psychologically healthy men with realistic expectations, who have had the benefit of full, frank and complete disclosure, will be pleased with their results.
Several categories of patients seek phalloplasty:
- Those with true penile hypoplasia ;
- those with marginally small or low normal penises with poor self-esteem ;
- those who have suffered ridicule or humiliation ;
- those who desire enhanced sensation during intercourse ;
- those whose ability to practice their occupations – actors, models, dancers – might be enhanced;
- body builders and weight lifters whose penile size is not commensurate with their idealized vision of themselves ;
- and those, like other males having cosmetic surgery, who simply seek to improve their appearance.
Since July 6, 1992, we have performed 738 phalloplasties on 640 patients. Ninety eight of these were additional procedures, 36 for residual nod-ules and / or for asymmetric or excessive fat resorption. After initial suc-cessful girth enhancement, 62 patients elected to have a second or third girth enlargement. Twelve patients had girth only and 14 had length only. Twelve patients had initially been operated upon elsewhere. Six patients who had undergone lengthening before the weight device became available and who had developed excessive scar tissue, underwent a second lengthening procedure after we had the weight device. At least 6 of our patients, and probably more, have gone elsewhere for a revision. Five patients underwent simultaneous enhancement phalloplasty and insertion of a penile prosthesis.
Most patients were in their third and fourth decade. The youngest was 18 and the oldest 61.
On the initial contact, a receptionist delivers basic information including cost and answers questions. The candidate completes a detailed questionnaire regarding his medical, psychological, social, family and sexual history. Patients who smoke are encouraged to refrain from the time of the initial interview until 8 weeks after surgery. At the preoperative meeting with his surgeon, the patient undergoes a physical examination. Flaccid and erect measurements are recorded for length and girth and photographs taken. As circumstances permit, the erect measurement is done either after an injection of 7.5 – 22.5 mg of Papaverine or else with stretched length. The two methods of length measurement have been found to conform to within 0.65 cm. We invite the patients to ask questions. In the past year it has become our practice to ask the patient what he understands about the operation and what he expects its outcome to be. We strongly recommend this practice. It is by far the best way to correct misconceptions which the patient would otherwise carry with him into the operating room. We describe in detail the length and girth enhancement procedures. We show the patient how to use the weight device. He is told how to care for himself postoperatively. Finally, the patient reads and signs an extensive informed consent. He also reads and signs the position statement of the Society for the Study of Impotence of the American Urological Association which contains strong cautionary language. All patients receive a complete blood count, urinalysis and a standard chemscreen. Patients over 40 receive an electrocardiogram.
Operative Technique
How We Do It
The patient shaves his abdomen, genitalia and upper thighs before entering the operating room. General, spinal, or epidural anesthesia is used depending on the anesthesiologist’s and the patient’s preference and where the fat is to be harvested. Intravenous Gentamicin and Vancomycin are started 20 min before surgery. Before liposuction, the abdominal wall, flanks and pubic area down to the inferior pubic notch are infiItrated with a liter of buffered sterile normal saline containing 2 cc of 1/1000 epinephrine and 30 cc of Lidocaine
 Fig 7 • Subcutaneus spaces of abdomen, supra- and infra-pubic areas being infiltrated with saline – lidocaine, epinephrine, before harvest.
Fig 7 • Subcutaneus spaces of abdomen, supra- and infra-pubic areas being infiltrated with saline – lidocaine, epinephrine, before harvest.A vertical line is drawn from the middle of the base of the penis toward the umbilicus to ensure symmetrical flap design. An inverted V to Y advancement flap is made on the lower abdomen at the base of the penis within the pubic escutcheon (Fig. 8-10). Each leg of the V is usually about 4 cm long and the distance between the two legs at the base is about 5 cm. The base of the incision is placed 2 cm above the base of the penis to avoid creating « cheeks ». The resulting skin advancement is about 2.5 centimeters. Some surgeons prefer a Z-plasty ; we have found that an inverted V to Y provides equal advancement and takes less time.
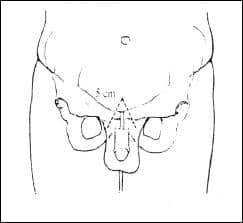 Fig 8 • Incision for advancement flap
Fig 8 • Incision for advancement flap Fig 9 • Advancement flap begun
Fig 9 • Advancement flap begun Fig 10 • Dissection of fundiform (superficial) ligament begun
Fig 10 • Dissection of fundiform (superficial) ligament begunThe dissection is carried down to the symphysis pubis. The second assistant retracts the penis caudad, bowstringing the attachments of the penis to the pubis. Richardson retractors are placed to protect the spermatic cords bilaterally and by exerting gentle lateral traction, the lateral extensions of Scarpa’s fascia are identified. The fundiform ligament and its lateral extensions are divided flush with the periosteum (Fig. 11).
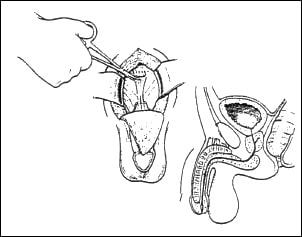 Fig 11 • Ligaments divided. Penile advancement achieved.
Fig 11 • Ligaments divided. Penile advancement achieved. The surgeon places a laparotomy pad over the dorsum of the penis and with his noncutting hand exerts pressure caudad against the dorsum of the penis. Behind the surgeon’s hand, and safe from the scissors, is the neurovascular bundle in the midline, covered by Buck’s fascia. Failure to maintain backward pressure against the penis allows the deep dorsal vein to enter the field and puts it at risk. Using blunt and sharp dissection the suspensory ligament is isolated and cut with all lateral extensions, flush on the periosteum. The dense areolar tissue beneath the suspensory ligament is freed from the pubic periosteum by blunt dissection, and carried medially and laterally for about 1.5 cm. When the free edges of the inferior symphysis and pubic rami can be palpated, the dissection is complete. The deep dorsal penile vein and its triturcation can be seen beneath the inferior pubic notch. Great care must be taken not to cut these veins ; if bleeding occurs, exposure may not be adequate for ligation, and the bleeding may be too much for the cautery. In this difficult circumstance hemostasis can reliably be achieved by wrapping large squares of gelfoam in a sheet of Oxycel, soalving this in thrombin, coating it with Avitene, wedging the plug into the space and maintaining pressure for 15 min. Ordinary hemostasis such as oozing from the periosteum is easily accomplished with the cautery. Meticulous hemostasis is essential to prevent postoperative problems. Hematoma beneath the flap or blood dripping down and causing scrotal swelling is distressing and delays resumption of normal activities. Before closing, we ask the anesthesiologist to lighten the level of anesthesia, to raise the patient’s blood pressure to preoperative levels, in order to identifv even slight oozing. Scissors lipectomy of the « V » flap and the suprapubic fat pad is performed. The flap is handled gently. We avoid putting sutures into the tip or squeezing the tip with the forceps. It should not be thinned excessively nor deprived of its blood supply. A dry laparotomy sponge is tucked into the infrapubic space while we proceed to girth enhancement. Attention is now directed to harvesting the fat.
Girth Enhancement
Harvesting : Abdomen (Fig. 12 – 14)
Liposuction is performed through the opening provided by creating the flap. The right-handed surgeon stands on the patient’s right side. A number 6 cannula is used and the suction machine (Wells Johnson Co., Tucson, AZ) is set well below maximum. Depending on the size of the penis and the patient’s wishes, between 30 and 60 cc of fat are harvested. The earliest aspirations are the least traumatized, contain the least detritus and are the most desirable. An endometrial curettage-type fat trap is used, with a funnel-shaped filter (Milex Corp., Chicago). Aspirated fat is scraped off the filter with a scalpel handle onto four folded sheets of sterile filter paper and gently pushed back and forth over the paper’s surface so that saline, blood and tissue juice will be absorbed and detritus identified and separated. We do not wash the fat. The clean, moist fat is stored in 30 cc syringe cylinders which stand up right, in a metal beaker containing sterile ice.
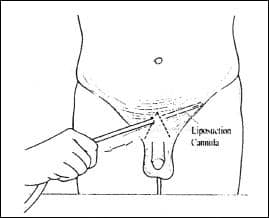 Fig 12 •
Fig 12 •  Fig 12 & 13 • Suprapubic and abdominal far harvest begun
Fig 12 & 13 • Suprapubic and abdominal far harvest begun Fig 14 • Left : Harvested fat scraped from tissue trap. Central : Sterile filter paper used to absorb fluid. Right : Fat stored in 30 cc syringues in ice slush, until injection
Fig 14 • Left : Harvested fat scraped from tissue trap. Central : Sterile filter paper used to absorb fluid. Right : Fat stored in 30 cc syringues in ice slush, until injectionHarvesting : Buttocks
When the patient’s abdominal donor site lacks insufficient fat, we usuallv defer surgery until he gains 4.5 – 6.8 kg, or else perform a DFT. Occasionally, we will harvest fat from the buttocks. Even in spare, lean young men with concave buttocks, the buttocks almost always yield 60 cc of at least fair quality fat. In these cases, the patient receives an epidural or spinal anesthesia so he can assist in the turning process. If general anesthesia is used, intubation is required. One-half liter of the saline / epinephrine / lidocaine solution is infused into each buttock, flank and medial thigh. Liposuction is carried out through a one mm. inferolateral incision in each buttock. The incision is closed with a single 2-o chromic catgut suture, covered by a Steri-strip and the patient is turned supine again.
Fat Injection (Fig. 15 – 17)
A 16F Foley catheter is inserted to avoid urethral injury. The righthanded surgeon moves to the patient’s left side. The assistant pulls the penis caudad and using Adson-Brown forceps he and the surgeon grasp a thin fold of loose skin in the coronal suIcus. A 2-port 13-cm fat injection cannula (Welis Johnson, Tucson, AZ) is bluntly thrust through the skin fold into the subcutaneous dartos fascia on the dorsal midline of the shaft. The subcutaneous space on the penile shaft normally is trabeculated into compartments by the dartos fascia, lymphatics and blood vessels. To inject fat smoothly and uniformly and minimize clumping, these compartments must be made to communicate freely.
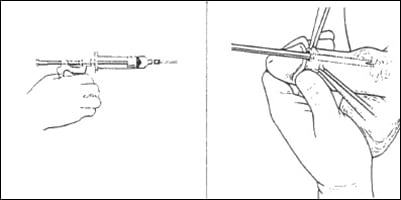 Fig 15 •
Fig 15 • 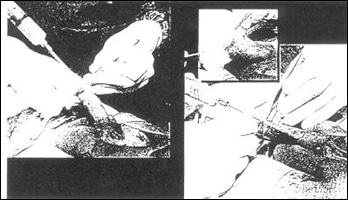 Fig 16 • Fat injected into subcutaneous space of penile shaft
Fig 16 • Fat injected into subcutaneous space of penile shaft 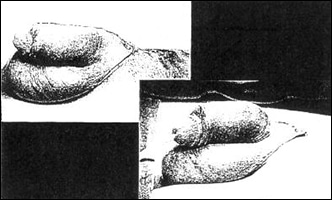 Fig 17 • Fat injection completed. Smooth symmetrical girth enhancement achieved. About 50% of the fat remains permanently.
Fig 17 • Fat injection completed. Smooth symmetrical girth enhancement achieved. About 50% of the fat remains permanently.Through a single penetration, using a back and forth motion trom the coronal sulcus to the base, the blunt cannula is repeatedly thrust and withdrawn everywhere except over the urethra. This dissection must be carefully done. This is not the place to hurry. The cannula will harmlessly slide oft vessels and lymphatics without injuring them. After free communication has been established throughout, the fat is injected. A grease-gun type injection syringe (Byron Medical, Tucson, AZ) with one of the cylinders containing the fat is attached to the cannula, and the fat is injected beginning with the cannula tip at the base of the penis and withdrawing it toward th entry point. If adequate dissection has been accomplished and all spaces communicate, usually only one injection site is needed. Sometimes, more laterally, a second, or rarely, a third entry is needed. How much fat to inject is determined by the patient’s wishes, the availability of quality fat, the looseness of the skin, the overall size of the penis, especially the glans, and the certain knowledge that excess fat will clump and degenerate. Some surgeons use a rubber band around the base of the penis to avoid perforating Buck’s fascia posteriorly with the cannula.
Injected fat tends to collect at the base and in the frenular area where the skin is loosest. It can be manually molded into a more symmetrical cylinder and held in place with a dressing. Before edema starts to occur the penis is sprayed with a liquid adhesive and then wrapped snugly but not tightly with a sterile ganze (Kling) dressing, which helps to mold the fat and hold it in place until it takes. A sterile Coban is applied. The penis wrap is not an afterthought. It is an important part of the operation. If the dressing is too loose, it will slide off ; if too tight, nocturnal erections will be uncomfortable and ischemia and even necrosis may occur.
Closure (Fig. 18 – 20)
Before starting the closure we again inspect the infrapubic space for hemostasis. Using 2-0 Vicryl interrupted sutures, the remnants of the fascia and areolar tissue just beneath the pubis are brought together in the midline. Several bites are taken attaching the deepest layer of the dermis and Buck’s fascia at the base of the penis to the proximal tunica albuginea. This pulls the skin at the base of the penis backward, defining the penile-scrotal crease and adding apparent length to the shaft. Beginning at the apex of the « V », the incision is closed from side to side in lavers with 3-0 Vicryl until some resistance is felt. The « V »-shaped flap is then sutured into the remaining tissue defect with 3-0 Vicryrl sutures. At the confluence of the three lines of closure, the blood supply is precarious at best. It is well to avoid placing sutures in the very tip and the flap must be handled tenderly. If the tip of the flap is redundant, it is excised and discarded. The skin is closed with subcuticular 3-0 Vicryl. Meticulous attention must be paid to the closure. It will be subjected to the most minute scrutiny by the patient. No drain is used. A dry sterile dressing is applied. The catheter is removed. An abdominal binder is applied.
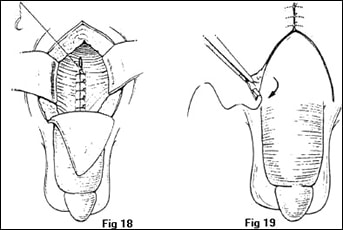 Fig 18 • Closure begun – Fig 19 • V-Y incision closed in three layers. Sucutilar skin structures.
Fig 18 • Closure begun – Fig 19 • V-Y incision closed in three layers. Sucutilar skin structures. Fig 20 • Closure completed
Fig 20 • Closure completedPostoperative Care
On the day after surgery we remove the wrap and inspect the penis. Any asymmetry or clumps can easily be smoothed out with gentle molding. We then rewrap the penis. The patient receives Ciprofloxacin 500 mg twice daily for one week. The abdominal binder comes off in a week, the penile and incision dressings in 10 days. The patient refrains from abdominal stretching maneuvers and intercourse for 6 weeks. For the first tew nights the patient deals with uncomfortabie erections by keeping two ice bags beside his bed which he uses when necessary. Diazepam 10 mg taken at bedtime will usually control nocturnal erections. Three to four weeks after the operation he begins using the weight device.
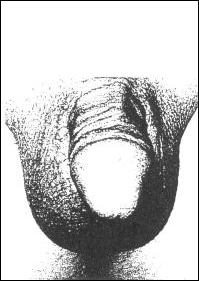 Fig 21 •
Fig 21 • 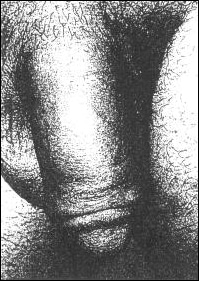 Fig 22 •
Fig 22 • During the first 6-8 weeks after surgery, about half of all injected fat is reabsorbed. As reabsorption takes place about 15% of patients report asymmetry or a residual lump. Patients are told before surgery that after they remove their dressing they should palpate for lumps every few days. Any palpable lump should be squeezed firmly between thumb and forefinger and it usually will disperse. If they delay too long, or if the lump is not fat but tissue debris it will not dissipate. Most patients with an otherwise pleasing result are content even if a small lump exists. Others are devastated at even the tiniest nodule or contour irregularity and the surgeon should be prepared to remove it or to add fat to smooth out the contour. Other infrequent complications include hematoma beneath the flap and in the scrotum, fat extravasation, infection, necrosis of the tip of the flap, partial wound separation, pain lasting longer than 48 h, hypertrophic scar, urethral perforation and dysuria.
When patients are measured on the operating table after surgery, with few exceptions they have gained at least 2.5 cm and often up to 4.3 cm in length. Soon thereafter, unless the weight device is used, retraction will commence, with variable loss of length. As soon as the patient began to use the weight device as instructed, retraction ceases. SIowly, over the next few months the penis elongates as the weight device acts as a tissue expander. If patients wear the weight device intermittently as instructed for 4 months after surgery, the great majority will gain at least an inch in length. Many patients will wear their weight devices for months or even years, sometimes adding extra weight, and will continue to gain length.
Girth gains are more variable and less predictabie. After 8 weeks about half the fat has already been reabsorbed and within the first year another 5% – 10% may be lost. Most patients remain with a girth gain of between 2.5 – 5.0 cm. We have followed some patients as long four years. In general, what they have after a year is what they will retain.
Around 12% of patients undergo a second operation for
- scar revision
- lump removal or contouring or
- additionai girth. Thin patients sometimes must gain weight before under-going reoperation.
When we reported our first 162 patients in 1994, overall patient satisfaction averaged 5-6 on an ascencling scaie of 1 – 10. We now judge patient satisfaction to be around 7. Unlike our earlier series when detailed questionnaires were mailed and telephone calls placed to all patients by an independent research team, we have this time by necessity relied on information gathered at postoperative visits and telephone calls. Patients often live at a distance and don’t return or call unless they have a problem. Our information, therefore is anecdotal and probably skewed toward the less favorable. Our experience has shown that this is probably the best we can do.
When asked retrospectively if, knowing what he knows today would he chose to have his operation again, 10% said no (sometimes vehemently), 15% were undecided, and about 75% again said yes. As before, no patient reported erectile loss. No patient reported instability of the base (swiveling) or lower erectile angle. Subsequent weight loss did not seem to compromise girth gains.
As near as can be determined, our infection rate is probably around three percent, none within the last 12 months. Early reports of « pus leaking out », without other symptoms were probably attributable to seepage of excess fat. Infection in the new penile fat is a serious complication and is associated with significant psychological and physical morbidity. The infectious agents were staph.epidermidis and the enteric organisms. These have without exception cleared with Ciproflaxacin but before they subside much of the transplanted fat may be destroyed, requiring reoperation.
To these young healthy men even a small hematoma in their scrotum is alarming. But large or small these all clear with heat and rest and time, but instead of the patient returning to work in 2 or 3 days, he may return in 2 or 3 weeks.
Discussion
With experience we now insert much less fat then previously. We have come to believe that less is more. Fat that is sequestered in masses which cannot be penetrated by revascularization will not survive. If it is gentIy harvested, tenderly treated, transposed to an adequately prepared and vascularized recipient site, and properly immobilized, fat survival will very likely be adequate. The literature states that dermal fat grafts should not exceed 1.5 cm in thickness. Assuming that the graft is circumferential, this means that dermal fat grafts can add about 3 cm to the penis girth. In our experience about the same is true for autologous transplanted fat.
Enhancement phalloplasty is not a perfect operation and potential patients must be aware of its limitations. We agree with Alter that penis enhancement techniques continue to evolve and results are constantly being evaluated. The same can be said for a great many common surgical procedures. Penis enhancement surgery can be performed with low morbidity and a high degree of patient satisfaction.
SHELDON O. BURMAN and THOMAS P. KELLY