
International Journal of Aesthetic and Restorative SurgeryVolume 2, Number 2, 1994, Pages 89-96
PENIS LENGTHENING
A new method of penis lengthening has been used in treating more than 260 cases of underendowment (cases 70-170 reflected in this report). The technique can be used to obtain a satisfactory cosmetic result by achieving normal size in micropenis, postoperative chordee, hypospadias and epispadias, or can provide a functional stump in the mutilated or traumatically amputated penis. The operation procedure is carried out in two stages : (1) A skin flap is raised in the pubic area and Iysis of the suspensory ligament between the penis and the pubic arch is performed while the penis is in a pharmacologically induced erection. (2) The penis is fixed in the new forward position and the new length is then covered by advancement and rotation of the skin flap. On average between 3.5 cm and 5 cm lengthening can be obtained. No permanent loss of sensation or erection ability occurred, while less than 2% of patients contracted infection. In all cases the result is an aesthetically acceptable penis that functions normally.
INTRODUCTION
Is penis length important ? Judging by the overwhelming reaction from underendowed patients to a new method of penis lengthening has elicited in the past year, the answer must be yes. Reports in the international news media on the development of this new technique have initiated an ava’anche of enquiries from the UK, USA, Western Europe (including Scandinavia), and from as far afield as the Far and Middle East, Africa, and Atlantic and Pacific Islands.
Sex and marriage counsellors may have largely played down physical shortcomings 1 in lieu of psychological solutions up to now, but the number of patients desperate to procure penis elongation and their tales of social maladjustment, fear of relationships and lack of self-confidence due to underendowment seem to indicate that a significant percentage of men experience penis size as a definite source of anxiety.
This does not suggest that the rectification of a physical shortcoming may miraculouslv banish psychological problems or that sexual performance replaces caring, nurturing, and sensitivity to a partner’s needs in a relationship. In fact, we strongly recommend that patients elected for penis lengthening simultaneously undergo psychological counselling to help undo a lifetime of established insecurities and destructive relationship patterns. What we have seen, however, is that addressing the source of anxiety an undersized penis can help the patient embark on the road to the recovery of a healthy self-image which may have positive repercussions not only in the sexual, but in all aspects of his life.
The average adult penis (1, 2, 3) varies in length between 7.5 and 10.5 cm in the flaccid state and between 12 and 18 cm erect (1), with a mean of 13 cm 3. A penis size below two standard deviations (i.e. below 10 cm in erect length) is regarded as a true micropenis (3). It goes without saying that ethnological and social factors mas also determine acceptable penis size in a specific community.
In more primitive communities for instance, penis size may take on a largely svmbolic representation of the importance of fertility and the continuity of life-cycles, while in general, average penis size will obviouslv correlate with the other physical attributes of smaller-built people. Sometimes remnants from our ancient past may persist in the collective unconscious of even the most modern civilized nations, represented in the myth of male superiority and expressed in social measures designed to suppress women (an indicator being the relatively late date at which women attained the vote in most of the civilized world).
Indications for penis lengthening surgery include micropenis, traumatic loss of part of the penis length as well as surgically corrected hypospadias epispadias, and chordee.
Psychological small penis or Small Penis Syndrome (4) describes the male presenting with a psychological anxiety over penis size. which in extreme cases may be expressed in pathological tendencies (such as self-castration or attempted suicide). Although psychological counselling may often benefit such patients, self-image is sometimes so severely affected that surgerv may be indicated to correct their concern (5).
A recent report suggests that augmentation mammoplasty patients often suffer from underlying psychopathology (6). After surgery the majority of these female patients function better (psycho-)sexually, show reduced levels of anxiety and depression and generally feel much better about their bodies. Though no such studies have yet been undertaken among males with a poor self-image due to socio-psychologically unacceptable penis size, it seems likely that the same cause-and-effect pattern may exist.
MATERIALS AND METHODS
From April 1993 to March 1994 we performed our penis lengthening technique in more than 260 cases. lnitially we used the operation method described by Prof. Long Dao Chou from China (7), but later adapted it by revising the flap to better suit the Western male, who usually presents with more fat in the subcutaneous pubic area and by changing the technique of stitching the penis in its new position. Since switching to the new technique, we obtained an even greater increase in the average lengthening results, while the new method also ensures that the angle of erection does not change as with the original technique.
For the purpose of our study, we examined one hundred cases (from number 70 to number 170). Initial changes in the technique described by Prof. Long and a follow-up period of at least 4 months on the last patient represented here warranted this distribution of cases.
The consultation
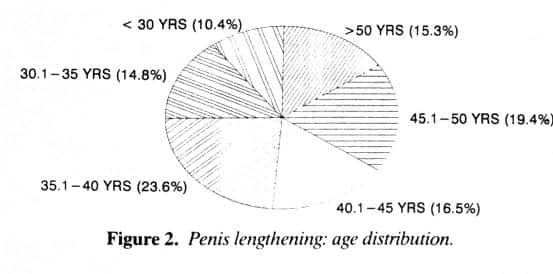
The reasons cited by our patients to obtain penis lengthening surgery varied from a poor self-image to traumatic amputation of the penis (Fig. 1). The age distribution of our patients is shown in Figure 2, with the majority of cases (59.3%) falling within the age group 30-50 years.
PENIS ELONGATION REASONS
– Traumatic : 1% – Congenital : 6% – Functional : 14% – Self-Image : 79%
Some important aspects to consider during consultation with a patient requesting penis lengthening surgery are :
General health. Cigarette smoking poses a significant danger to skin flap survival in the post-operative period. Flap sloughing, especially at the apex of the skin flap, occurs almost without exception only in patients who continue to smoke in the post-operative period. Medication (anti-depressants, hyperten-sive treatment) might have an influence on erection ability. Previous operations could have left scars in the area of the skin flap. This will endanger flap survival.
Sexual function. It should be made clear to the patient that a longer penis may not necessarily lead to a better sex life 1. He should understand that orgasm in the female is not dependent on deep penetration. Unless the penis is a true micropenis, the increased length will not lead to more stimulation in the female partner. A patient with a history of impotence requires special consultation. lt should be stated clearly to the patient that the penis lengthening operation has no effect on anatomical impotence. Should impotence be ascribed to a negative self-image because of penis size, however, the patient might benefit from this procedure.
PENIS ELONGATION AGE GROUPS
ANATOMY OF THE PENIS
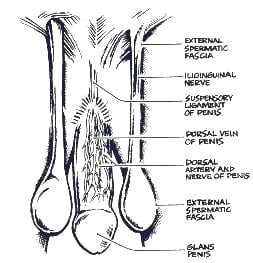
The penis consists of the corpus spongiosum, which contains the urethra, and the two dorsally situated corpora cavernosa (Fig. 3).
The root of the penis originates from the perineal membrane in the area below the subpubic angle. Here the bulk of the penis (corpus spongiosum) is attached to the undersurface of the perineal membrane. The bulk is joined by the crura (corpora cavernosa) to form the free penis.
All the corpora are enclosed by the deep fascia of the penis (previously called Buck’s fascia). Under the deep fascia of the penis, on either side of the deep dorsal vein, run the dorsal arteries (derived from the hypogastric artery through the internal pudendal artery) of the penis, which supply the skin, fascia, and glans with blood. Further blood supply to the penis is derived from a branch of the internal pudendal artery which supplies the corpora cavernosa. An artery to the bulb supplies the corpus spongiosum and the glans. The deep artery, derived from the internal pudendal artery and supplying the corpora cavernosa, is responsible for erection.
Venous return from the corpora is partly by (a) veins that accompany the arteries into the internal pudendal veins ; (b) the deep dorsal vein, which pierces the triangular suspensory ligament to drain into the prostatic venous plexus ; and (c) the superficial dorsal vein, which collects blood from the dorsal skin of the penis before draining into the superficial external pudendal and saphenous veins.
The lymphatic drainage of the penis consists likewise of a superficial and a deep system which follows the venous drainage. The nerves of the penis are derived from the spinal and autonomic systems. The dorsal nerves of the penis, which are situated laterally to the dorsal arteries under the deep fascia of the penis, serve the dorsal and lateral skin and the glans of the penis (Fig. 5). The erectile bodies are enervated by the parasympathetic autonomic system (nerves erigentes). Ejaculation is initiated by the sympathetic hypogastric nerves.
Suspensory ligament
The suspensory ligament (Fig. 3 and 4) of the penis is of the utmost importance in penis lengthening surgery. This triangular sheet of fibrous tissue blends with the deep fascia of the penis and suspends the penis from the pubis where it emerges from beneath the symphysis pubis.
Its shape and extension is three-dimensional and stretches from the linea alba dorsally along the midline to the center of the penis. There it fans out laterally around the dorsum of the penis to encapsulate at least the dorsal half of the penis.
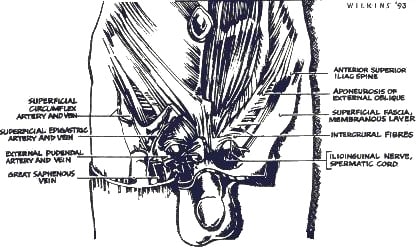
Anatomy of the pubic skin area
The anatomy of the pubic skin area (Fig. 4) is important as it supplies skin for coverage of the new penile length. Elevation of the dome-shaped skin flap which will cover the new penile length neeessitates division of superficial inguinal branches of the femoral artery and great (long) saphenous vein. The spermatic cord and ilio-inguinal nerve passing through the superficial inguinal ring is situated laterally in the approach to the suspensory ligament of the penis.
OPERATION TECHNIQUE
Though not strictly necessary, we recommend the cooperation of a plastic surgeon and a urologist in this operation, as there are two distinct parts pertaining to these two specialized fields. ln our experience, some patients presented with either additional urologenital problems such as malformation or dysfunction, which could best be treated by a urologist, or traumatisation or scars from previous surgery, which necessitated innovative flap design and cosmetic solutions and could best be treated by a plastic surgeon.
Post-operative treatment also falls into these two categories, for instance urinary retention, sustained erection, transient sensation loss in the dorsal nerve area, temporary diminished erection ability, endangered flap survival, infection, sloughing, or aesthetic appearance.
We found it most practical and productive for the urologist to perform the extensive dissection of the suspensory ligament from the symphysis pubis without harming the dorsal nerves, arteries and veins, while the plastic surgeon undertakes the design and excision of the skin flap and the re-attachment of the penis to the soft tissue and lateral skin flaps and the closing of the wound.
With the patient in the supine position under general anaesthesia, the penis is injected with 20 mcg of Prostaglandin E1 (Prostin, Upjohn) into the corpus cavernosum. This creates an erection which greatly facilitates the operation, as it clearly defines the penile structures during the suspensory ligament dissection.
The erectile tissue also facilitates movement of the penis from under the symphysis pubis after suspensory ligament lysis and provides (due to this erectile tension) a firm layer of deep fascia by which to anchor the penis in its new position.
With a suitable working device, a line is drawn from the middle of the base of the erect penis in the direction of the umbilicus. This line ensures a symmetrical flap design. The skin flap outline is then drawn (Fig. 5a). The base of the flap is at the penis base with the penis diameter dictating the broadness of the flap. The flap is conical in shape and approximately 4 cm long. Pre-infiltration of the flap outline with a suitable vasoconstrictive agent reduces bleeding.
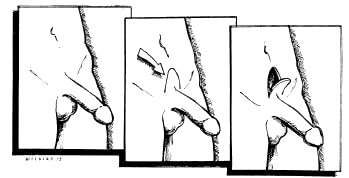 Fig 5a, b, c • Operation technique : a) erect penis ; b) design of skin flap ; c) elevated skin flap
Fig 5a, b, c • Operation technique : a) erect penis ; b) design of skin flap ; c) elevated skin flap
A combination of sharp and blunt dissection is used to gain access to the suspensory ligament (Fig. 5b, c). All the superficial inguinal branches of the femoral artery and the great (long) saphenous vein are cauterised and divided. Great care should be taken to isolate the flap without unnecessary thinning of the subcutaneous tissue or tension on the flap.
With adequate exposure, the suspensory ligament is divided, taking great care not to damage the dorsal nerves, arteries and veins of the penis. Usually these structures can be clearly identified once the central attachments of the suspensory ligament are divided from the suspensory ligament. Extensive dissection of the suspensory ligament from the symphysis pubis allows the erect penis to move approximately 9.5 cm forward. The subcutaneous soft tissues on either side of the penis is then approximated towards the midline and sutured with 2-0 Maxon (Davis and Geck) absorbable sutures. Care must be taken to avoid injury to the spermatic cords and ilio-inguinal nerves.
Approximation of the soft tissue obliterates the dead space that results when the suspensorv ligament is divided and creates a forward push on the penis where it emerges from the symphysis pubis.
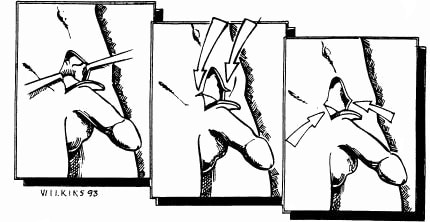 Fig 6a, b, c • a) exposure of suspensory ligament, b) lateral skin cutbacks, c) excision of triangular skin segments.
Fig 6a, b, c • a) exposure of suspensory ligament, b) lateral skin cutbacks, c) excision of triangular skin segments.
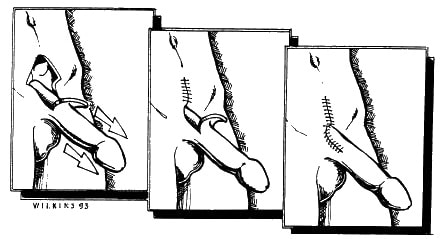 Fig 7a, b, c • a) Cutbacks allows foreward movements of penis, b) start of skin closure, c) complete skin closure
Fig 7a, b, c • a) Cutbacks allows foreward movements of penis, b) start of skin closure, c) complete skin closure
This provides more effective length as it straightens the natural upward curve of the penis.
It has been reported that approximation of the soft tissues prevents the penis from moving back under the symphysis (8). We doubt that this occurs, since we have experienced cases where relapse of penile length oecurred if the penis was not re-attached to the soft tissues and skin flaps.
Once the urologist has completed dissection of the suspensory ligament, the plastic surgeon prepares the lateral wound edges. Cut-backs are made (Fig. 6b, c) bilaterally into the skin edges and the small skin triangles next to the penis base are excised. These cut-backs prepare the space into which the skin flap will be rotated onto the new penis base (Fig. 7a-c).
The first suture to approximate the skin edges towards the midline and to pull and hold the penis into its new position is then closed. This suture is placed bilaterally through the deep fascia of the penis and through the dermis of the skin on either side of the wound.
After executing the first stitch, the skin flap is sutured into the defect. Subcutaneous approximating 3-0 Maxon absorbable sutures are used and the skin is closed with a continuous running 3-0 Nylon suture, which must be removed after 10 to 14 days.
The re-attachment of the penis to the lateral skin flaps ensures the formation of a new suspensory ligament which holds the penis in its new forward position and ensures the stability of the new penis during erection.
POST-OPERATIVE TREATMENT
Post-operatively, one day’s hospitalisation is required. We recommend two weeks’ sick leave (one week complete rest) and at least four weeks’ abstinence from sexual intercourse.
Our patients receive a course of cephalosporin antibiotics with sufficient coverage against gram negative and coliform organisms. Antibiotic ointment is applied to the wound area to keep the incision moist and helps to screen the wound from auto-contamination. Diazepam (10 mg) administered at night for three weeks has proved sufficient to control nocturnal erections. We have found that systemic oestrogen preparations produce undesirable side-effects and recommend caution when used.
Due to the advancement and rotation of the skin flap, an area of skin approximately 3-5 cm in length and containing pubic hair covers the dorsum of the proximal penis (Fig. 7e). Many patients regard this as an added sexual stimulant to their female partners, while some opt for removal of this hair by electrolysis.
RESULTS
As reflected in the accompanying graphs covering the 100 patients (number 70 to number 170), the average penis length increase was from 11 cm to 15 cm (Fig. 9, 10). This can be regarded as the transformation of an undersized penis into a penis of normal length.
PENIS ELONGATION PRE-OP LENGTH
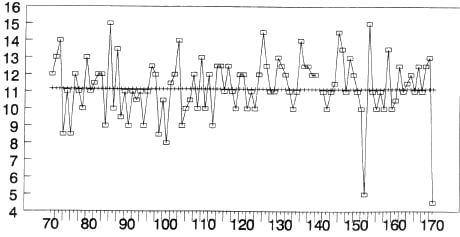 Fig 8 • Average pre-operative penis length (erect)
Fig 8 • Average pre-operative penis length (erect)
PENIS ELONGATION LENGTH INCREASE
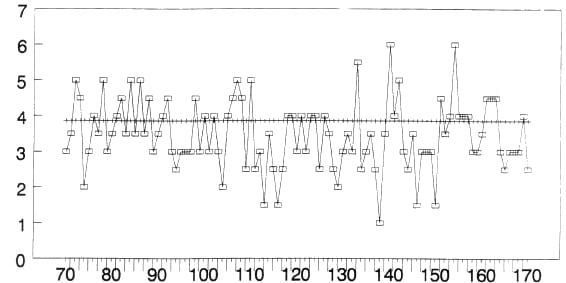 Fig 9 • Average lengthening increase (erect)
Fig 9 • Average lengthening increase (erect)
None of our patients complained of a change in the angle of erection after surgery and we received no reports of loss of erection ability. Transient partial neuropraxia in the distribution area of the dorsal nerve of the penis, lasting 8-12 weeks, occurred in three out of 260 cases. (See photographs depicting pre- and post-operation penis length in erection Figs. 10, 11 and 12).
 Fig 10 •
Fig 10 • 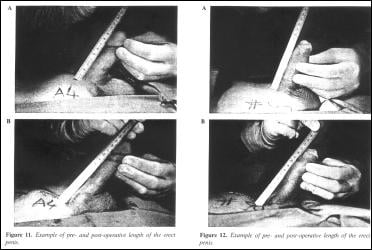 Fig 11 & 12 •
Fig 11 & 12 • COMPLICATIONS
Though complications are minimal with this technique, the following have occurred and may be treated as indicated.
Persistent erection
A sustained erection resulting from Prostin injections should be recognized and treated early on as this condition may lead to impotence. Priapism (an erection lasting longer than 6 hours) can be reversed by the injection of 0.3-0.5 ml of a 1000 mcg/ml solution of Phenylephrine into the corpus cavernosum (9). We have experienced this in only three patients in our series of 260 cases.
Urinary retention
Urinary retention has occurred in two of our cases so far. Catheterization for 24 hours proved effective in solving this problem.
Infection
In our first 260 cases, we had to treat four patients for serious infection. Streptococcus faecalis (two cases), pseudomonas aeruginosa and acinobacter was cultured and treated accordingly. Should disruption of the wound occur, as happened in these cases, resuturing of the wounds must be attempted as soon as the wounds are reads.
Skin sloughing
Skin flap sloughing is another major hazard and can be treated bv desloughing as an office procedure, followed by daily dressings with gauze, slightly moistened with an antibacterial solution. This complication occurred almost exclusively in men who smoke and we clearly warn our patients of this hazard.
Dorsal nerve injury
Direct injury to the dorsal nerve of the penis can result in sensation loss to the dorsum of the penis and glans. As stated previously, we have had three cases where transient partial sensory loss occurred in the distribution area of the dorsal nerve. This improved in 8 to 19 weeks.
DISCUSSION
The patients represented in our series are from all walks of life and range in age from pubertal to septuagenarian, though most fell in the category of 35 to 50 years. The majority suffered from congenital underendowment. Others had small penises following previous operations, trauma, mutilation or chordee. In some cases the undersized penis was obviously a hereditary problem.
Interestingly, most heterosexual patients confessed that their fears and anxieties about tneir penis size had sprung not from the reaction of woman during sexual relationships, but from the denigrating behaviour of other males. Moreover, women generallv do not require deep penetration for sexual satisfaction, since only the outer third of the vagina is richly endowed with sensory nerve endings.
ln most cases psychological problems resulting from underendowment seem to have been rooted in childhood, when adolescent boys inevitably find themselves exposed to physical comparison and sexual boasting in the locker room situation, or subjected to the mostly well-meaning but potentially devastating reaction of concerned fathers who perhaps attach too much importance to physical size themselves. The feelings laid down during this sensitive period of budding sexuality and developing self-esteem seem to persist into adulthood with paralyzing effects if not addressed positively, obviously the earlier the better.
The psychological importance of penis lengthening is underlined by the fact that the operation does not necessarily improve sexual function or performance. and does not cure anatomical impotence. Nevertheless, the many patients who have requested the operation and their almost unanimous positive response to the end result prove that penis size is a determining factor in the social emotional and psychological development of a sizeable percentage of underendowed men.
HENNIE ROOS *, IRVING LISSOOS **
REFERENCES
- Green R: In Human Sexuality. Baltimore : Williams and Wilkens, 1975; 99-23.
- Winter JSD. Fraiman C: Pituitary gonodal relations in male children and adoles-cents. Pediatr Res 1972; 6:126.
- Teaguc JL. Gonzales ET: The many difficulties of managing micropenis. Contemp Urol 1993; 5:15.
- Murtagh J: The `small` penis syndrome. Aust Fam Physician 1989; 18(3):218-220.
- Clarkson P, Stafford-Clark D: Role of the plastic surgeon and psychiatrist in the surgery or appearance. BMJ 1960; 2:1768-1771.
- Schlebush L, Mahrt I: Long-term psychological sequelae of augmentation mammoplasty. S Afr Med J 1993; 83:267-271.
- Long DC: Elongation of the penis: Chung Hua Cheng Hsing Shoa Shang Wai Ko Tsa Chih 1990; Mar; 6(ii):17-9, 7 (Chinese).
- Kabalin JN, Rosen J, Perkash I: Penile advancement and lengthening in spinal cord injury patients with retracted phallus who have failed penile prosthesis placement alone. J Urol 1990; 144:316-318.
- Dittrich A, Albert K. Bar-Moshe O, Vanendris M: Treatment of Pharmacological Priapism with Phenylephedrine. J Urol, 1991; 146:323-324.
Note on the authors
* Hennie ROOS : Plastic surgeon, Johannesburg, South Africa, MMED (Stelle), FCS (SA), Fellow Cranofacial Centre, Paris.
** Irving LISSOOS : Urologist, Department of Urology, University of Witwatersrand, Johannesburg, FCS (SA), FRCS (Edin), FACS
Send correspondence to Dr HC ROOS, PO Box 441, Auckland Park, 2006 SOUTH AFRICA